


Ethics
This study was conducted in accordance with the declaration of Helsinki and was approved by the Bioethics Committee of the Nicolaus Copernicus University in Toruń at the Ludwik Rydygier Collegium Medicum in Bydgoszcz, Poland (KB 684/2019). All participants (N = 200) provided written informed consent and signed the extended note regarding study information, including information about data privacy and its pseudo-anonymization and anonymization for the purpose of analyses and publications related to the research project. The public database is now fully anonymized. After signing the informed consent, participants received their own results regarding genetic screening and psychometric scores. To avoid a bias in consecutive stages of the study, the results were handed out after the final experimental session. Participants included in the second stage of the study also received a cash remuneration (100 PLN, ~21 EUR) and their own MRI results. Additionally, we asked participants to declare if they wanted to receive the results of genetic tests (and other tests as well). Out of the 200 participants taking part in the study, 192 signed an addendum, agreeing to make the research data publicly available in the open scientific database – these data is described here.
General information
One hundred ninety two middle-aged individuals (50–63 years old) completed the first phase of experiments, and 79 participants continued the experiment through its second phase (Figs 1, 2, Table 1). The first phase of the experiment included genetic screening (only APOE/PICALM polymorphisms) and a meeting during which participants completed psychometric tests (see Fig. 1 and the next paragraph for a list of tests) and general, extensive questionnaires on health and demographic data. In the second phase of the experiment, subjects with risk alleles for APOE/PICALM genes and a matched group of subjects with neutral alleles were invited to participate in the neuroimaging sessions. EEG recordings and fMRI scans were performed on separate days. The EEG session was conducted in the EEG laboratory at the Nencki Institute of Experimental Biology PAS, and the fMRI session was conducted in the Bioimaging Research Center at the Institute of Physiology and Pathology of Hearing in Poland. An approximately equal number of subjects underwent an EEG session, followed by an fMRI session, and vice versa to avoid a task learning bias in either design (N = 31 EEG session was administered first, N = 39 fMRI session was administered first; the order is indicated in the database). During both sessions, we used a resting-state protocol, as well as two cognitive tasks, one examining broad executive functions (Multi-Source Cognitive Task, MSIT) and the other examining memory (Sternberg Memory Task). Blood samples for complete blood count (CBC), lipid profile and antibodies against herpes simplex virus (HSV-1) were collected on a separate day.
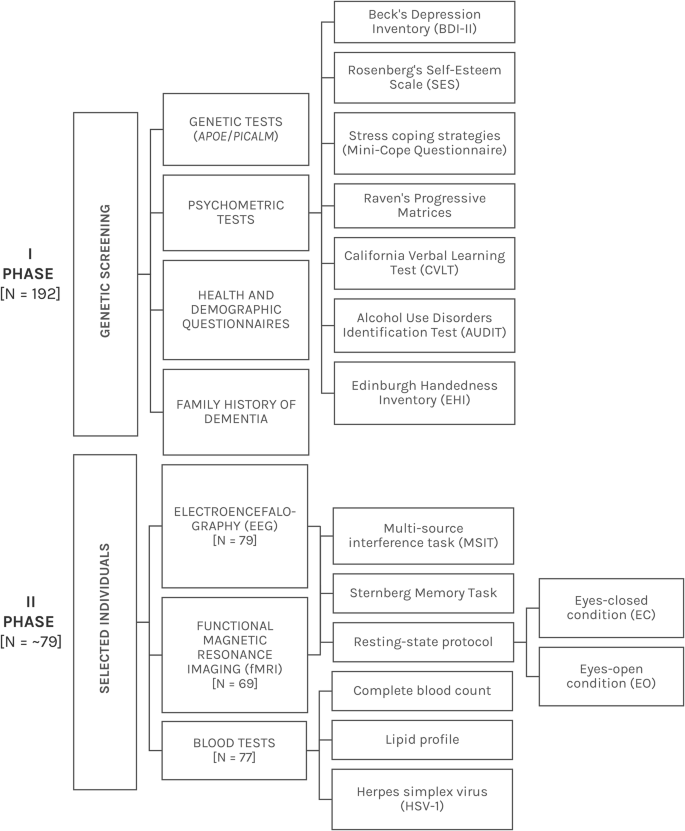
Diagram of the study methodology, which illustrates both study phases and conducted experiments. *The exact number of participants changed at different stages of the study. See the Missing data section for more information.
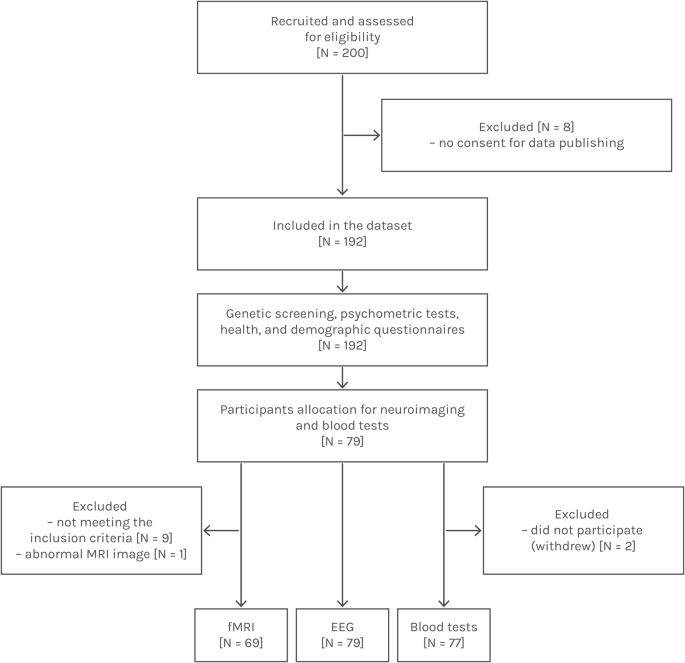
Flow diagram illustrating the study design, including participant selection and the quantity of data included within this open dataset.
The subjects were asked to stop taking medications 24 hours before the EEG study unless it was necessary in relation to a chronic condition. Subjects were also asked to refrain from consuming alcohol, stimulating and caffeinated beverages, and psychoactive substances 24 hours before the study. However, if it was natural for the subject to drink a cup of coffee in the morning, we asked them to maintain their natural daily rhythm. Subjects were asked to be well-rested before either session. The exclusion criteria for the study were as follows (the participants were asked about the exclusions during an initial online survey, some of the questions were additionally confirmed in the survey before fMRI sessions, and all of them were printed on the “Information about the study” sheet that was given to the participants before the first EEG or fMRI session for signing):
-
recent or ongoing infection,
-
general excessive health problems,
-
epilepsy,
-
known mental illness or brain damage,
-
chronic headaches,
-
sleep disorders,
-
skin diseases,
-
metal objects/implants in the body,
-
pregnancy.
Demographic, health and psychometric questionnaires
The demographic and health questionnaire included the following information:
-
Demographic data: age, sex, education level.
-
Health data: learning difficulties (dyslexia, etc.), body-mass index (BMI), diabetes, hypertension, thyroid diseases, other chronic diseases, allergies, permanent drug intake, nonsteroidal anti-inflammatory drugs intake, smoking status, caffeine intake, alcohol consumption (measured by AUDIT test).
-
Blood tests: leukocytes, erythrocytes, hemoglobin, hematocrit, MCV, MCH, MCHC, RDW-CV, platelets, PDW, MPV, P-LCR, neutrophils, lymphocytes, monocytes, eosinophils, basophils, total cholesterol, HDL cholesterol, non-HDL cholesterol, LDL cholesterol, triglycerides, HSV.
-
Additional data: session order (EEG/fMRI).
-
Genetic data: APOE haplotype, PICALM rs3851179 genotype.
-
Family history of dementia data (parents).
Participants filled in a battery of psychometric tests (Fig. 1), including:
-
Beck’s Depression Inventory (BDI): measured depression and mood changes. This widely used test consisted of 21 items that assessed various symptoms of depression/mood, such as sadness, guilt, fatigue or loss of interest. The total score ranged from 0 to 63. The database includes the final score for each participant36,37.
-
Rosenberg’s Self-Esteem Scale (SES): measured self-esteem and confidence. The test consisted of 10 statements that assessed both positive and negative feelings about oneself. Scores ranged from 0 to 30 points. The database includes the final score for each participant38,39.
-
Mini-Cope Questionnaire: measured stress-coping strategies used in daily life situations. The test consisted of 28 items. The database includes 14 basic items that could be further recalculated40,41.
-
NEO-FFI Personality Inventory: measured the personality traits known as the Big Five personality traits. The scale measured: neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness. The test consisted of 60 items. The database includes the final score for each measure42,43,44.
-
Raven’s Progressive Matrices (RPM) in standard/classic version: measured fluid intelligence and the ability to solve complex, novel tasks. We changed the time that the test subjects had to solve the test to 30 minutes (from unlimited time in the classic version)45,46.
-
California Verbal Learning Test (CVLT): measured memory abilities and verbal learning. The CVLT provided several measures, including total recall, recall by trials, recognition memory, and others. The test was ecological, meaning that the questions were related to daily activities, like memorizing shopping lists47,48.
Handedness inventory (all participants were right-handed)49.
All psychological tests were the Polish adaptation and standardized versions and were obtained from the Psychological Test Laboratory of the Polish Psychological Association. The health information included in the ‘demographic & health’ questionnaire was provided by the participants, so the answers were subjective and not medically verified (i.e., hypertension or diabetes).
Blood tests
Blood testing was outsourced to a third-party, certified medical laboratory facility. Samples were collected by a trained nurse in the morning at the local facility. HSV tests were performed using the ELISA method (Euroimmun kits), testing the IgG antibodies. The blood test laboratory norms for the performed tests are shown in Table 1.
Genetic screening
Genetic screening was outsourced to a third-party company (Genomed S.A., Poland). Buccal swab samples were collected by brushing a swab on the surface of the inner cheek (buccal mucosa) (we used COPAN eNat® buccal swabs especially designed for nucleic acid collection and long-term preservation). The risk gene APOE (rs429358/rs7412, needed for determining the main ε2, ε3, and ε4 variations) and PICALM (rs3851179) alleles were determined with the traditional Sanger sequencing protocol, which is a reliable, standardized DNA sequencing protocol. Genetic data frequencies are shown in Table 2.
Recording software and devices
EEG data was recorded with the use of the Brain Products systems: an actiCHamp amplifier and high-density actiCAP electrode caps with high-montage 128 electrodes included (Brain Products GmbH, Munich, Germany). Standard Brain Products electrode configuration files were used (Fig. 3). The online reference was set at FCz electrode, which can be easily recalculated to any desired off-line reference types, including the average reference. Real electrode localization was obtained with the use of a handheld CapTrak 3D scanner (Brain Products GmbH, Munich, Germany) at the end of each session. The lowest possible impedance was maintained during the recording, on average 5–10 kΩ, by gently rubbing the skin and by EEG gel application. The sampling rate was set to 1,000 Hz. No notch filters or high-pass filters were used during the recording, only the low-pass filter was used and set to 280 Hz.
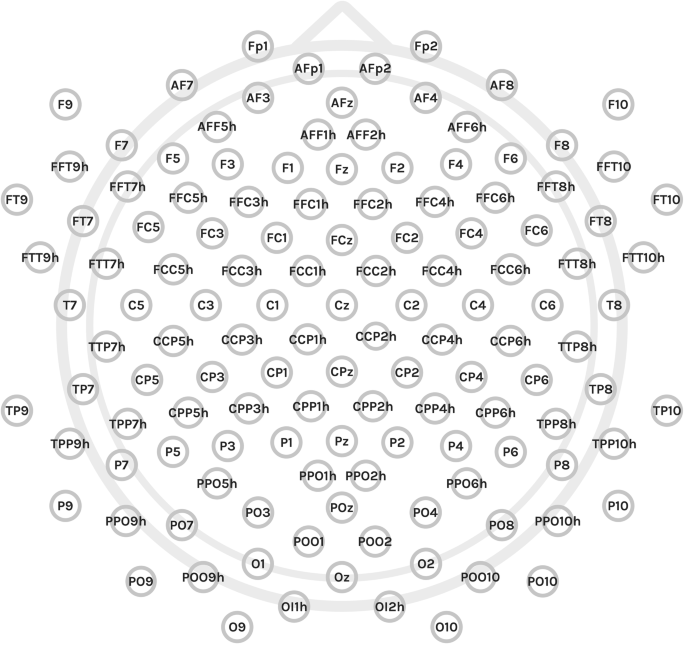
Electrode configuration used for the experiment (128 electrodes).
fMRI experiments were conducted with a 3 T Siemens Prisma FIT scanner (Siemens Medical Systems, Erlangen, Germany). The acquisition parameters were as follows: repetition time (TR)—0.8 s, echo time (TE)—0.038 s, slice thickness—2 mm, and voxel volume—2 × 2 × 2 mm. Images were taken with two-phase encoding direction: anterior-posterior (AP) and posterior-anterior (PA). Additional information on slice timing, echo train length, scanning sequence, variant and other options are included in the database in corresponding.json files and/or corresponding headers of *.nii files (NIfTI-1 Data Format).
Environment
First phase
The participants were recruited through conventional methods (e.g., posters, flyers) and online social media. For both methods, the individuals were directed to a website with information about the study and an online survey where the information about contraindications to participation in the study was indicated. Only subjects with no contraindications were recruited. The list of contraindications was shown to the recruited respondents during the first (psychometric and questionnaire) session and then again before the fMRI session where, again, we asked about MRI-relevant contradictions. The first phase of the study was conducted during individual meetings in a quiet, separate room. At the beginning, the subjects read the information about the study, signed that they had read the document information and signed the informed consent for the study. Then, a session of psychometric testing was conducted; all tests were completed by the subjects on their own, except for the CVLT test, which required researcher involvement. After the testing session, a buccal swab sample was taken for genetic testing (the subjects were instructed on how to take the sample on their own).
Second phase
The experiments were conducted in the morning and afternoon, with the possibility for the participant to choose the most convenient time of the session in order to be fully rested. Experimental procedure details are available in Table 3 for EEG and Table 4 for fMRI sessions. The tables include the order of each procedure and task and the estimated time. The high-density cap was prepared before each session to reduce the participant time required during EEG preparation. During the EEG session, the participant was sitting alone in a quiet room on a comfortable chair in front of a monitor. The study was supervised by the researcher sitting in another room via a remote desktop connection to the experimental computer and a LAN camera overlooking the EEG lab.
Data protection
Data anonymization is a process of removing or altering personally identifiable information from a dataset in such a way that the data can no longer be linked back to an individual. The purpose of anonymization is to protect the privacy of individuals while still allowing the dataset to be used for analysis and research. All data in the database were anonymized with special codes (sub-1, sub-2 etc.), and no direct personal information was maintained through all of the uploaded files. All metadata information related to participants was removed from neuroimaging files.
Task details
All tasks were written and performed within the Presentation software v. 20.050. Stimuli were displayed in gray color (RGB values: 206, 206, 206) on a dark background (RGB values: 58, 58, 58). The stimuli were displayed on a monitor during the EEG session and on goggles (VisualSystem HD, NNL, nordicneurolabs inc.) during the fMRI session, which also allowed researchers to see participants’ eyes and track their engagement in the task and their wakefulness. Markers used in the EEG files are described in Table 5.
Participants responded using a keyboard (Sternberg memory task) and numeric keypad (MSIT) during the EEG session and with a response grip (Smitlab response grip) during the fMRI session. Each file may also contain additional ‘boundary’ type markers that are added automatically by EEGLAB when the file is opened/saved (e.g., at the beginning of each file). In addition, these markers are added where a portion of files are concatenated or deleted. There was a short training session before the main experiment, during which the participants could familiarize themselves with the tasks. The training was repeated if the participants answered incorrectly until they understood the instructions.
Multi-source interference task (MSIT)
Multi-source interference task (MSIT) is a cognitive task used to measure adaptive control, cognitive control and cognitive interference51,52. The task measures the ability to ignore distracting information and focus on the task-relevant information. Participants are presented with a sequence of three digits (e.g., ‘331’), and they have to identify the target, which is a unique digit, while ignoring distractors (two other, identical digits) by pressing the button corresponding to the digit value, and not its position (in this example ‘1’ would be the correct answer). The digits can be displayed in a congruent way (congruent, low-demanding condition; i.e., the target digit value and its position are the same, which fastens the reaction time towards congruent trials, like ‘122’) or incongruent (incongruent, high-demanding condition; i.e., the target digit location and the response button location are not the same, which prolong reaction times, like ‘331’ trial); this manipulation creates cognitive interference. The MSIT is widely used in cognitive neuroscience research and has been shown to reliably activate the dorsal anterior cingulate cortex, medial prefrontal cortex, and supplementary motor area, among other described areas53. It has also been used in clinical populations to assess deficits in various disorders54,55 and in healthy aging56.
Sixteen sets of predefined stimuli sequences were prepared with the use of the OptimizeX genetic algorithm57 to reduce the collinearity in the event-related task design, especially for fMRI purposes58. Orthogonality of regressors in a general linear model (GLM) of fMRI analysis is needed to reliably estimate the results, as collinearity may impact the estimated contrasts of parameters and, thus, the obtained results58,59. Maximally 4 trials of the same condition were displayed in a row, and maximally 2 identical stimuli were displayed in a row. Out of 16 sets of stimuli, both conditions were correlated on a level of 0.14 in 3 designs, 0.16 in 3 designs, 0.17 in 1 design, 0.18 in 7 designs, and 0.19 in 2 obtained designs. The task was prepared in two runs, 83 stimuli per each run which lasted for ~4.2 minutes (with an equalized number of each individual trial, either 13/14 repetitions, therefore the number of trials per condition was also balanced; 166 trials in total; task lasted for ~8.5 minutes in total). The stimuli were displayed on the screen for 1,000 ms, and ISI varied between ~1,000–8,140 ms (on average: ~1,804 ms from all sets). A dark, blank screen was displayed during the interstimulus interval. In each run, a 10-second break, marked with ‘ + ’ was included in the middle of the run. The task design is shown in Fig. 4.
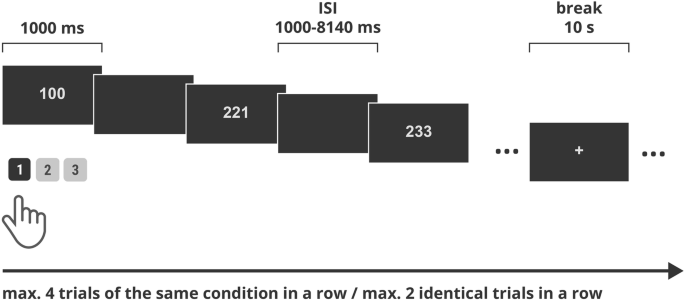
Multi-Source Interference Task design. ISI: interstimulus interval.
Note: During the initial part of the experiment, the MSIT task in fMRI was constructed without the rule of 4 same trials in a row; fMRI files that do not follow the rule: sub_01, sub_20, sub_33, sub_60, sub_78.
The list of possible trials included:
-
Low-demanding condition, congruent: 100, 020, 003.
-
High-demanding condition, incongruent: contingency-equalized design presenting each unique stimulus equally often; several parallel subsets of stimuli were used for different sets, either 221, 233, 131 or 212, 332, 311 or 313, 112, 322 or 331, 211, 232. For each individual experiment, a set of incongruent stimuli was randomly drawn to avoid a possible contingency learning bias60 that occurs in the original MSIT task. Information about the individual trials was stored in the logfile data (note that leading zeros are not saved; therefore, trial ‘3’ ->‘003’, ‘20’ - > ‘020’ etc.).
Sternberg memory task
The Sternberg Memory Task is a widely used psychological paradigm designed to investigate short-term or working memory processes. It was developed by Saul Sternberg in 196661 and has been used extensively in psychological and neuroimaging research. There are various procedures for performing the Sternberg task and studying different memory aspects, but in each instance, a participant is presented with a list of items and then with individual probes. The participants must indicate whether the probe item was part of the original list. Participants are required to respond as quickly as possible and as accurately as possible (without sacrificing accuracy for speed response). In the case of our procedure, the individual was presented with the strings of letters and then with single-letter probes and needed to answer if the letter presented was included in the string (by pressing the right arrow key on the keyboard during the EEG or the first button on the response pad during fMRI), or not (by pressing the left arrow key on the keyboard during the EEG or middle button on the response pad during fMRI).
Predefined letter combinations, containing only consonants, were used: 24 low-demanding memory sets including 4 letters (e.g., “K W + C F”, “P Z + D J”) and 24 highly-demanding memory sets including 8 letters (e.g., “R T G L + D F B Z”, “W T H J + C F L R”),. Three probes were presented after each memory set, and each included one letter from the consonant set (B, C, D, F, G, H, J, K, L N, P, R, S, T, W, Z). During the retention period, a “ + ” sign was presented on the screen. The interval between the probe presentations was set to the range of 800–1800 ms (in increments of 200 ms, e.g., 800, 1000, 1200, 1400, 1600 or 1800 ms); the interval between the whole trials (understood as a memory set, retention, probes) was set in the range of 1300–2800 ms (increments of 100 ms, e.g., 1300, 1400, 1500 ms etc.). Three breaks lasting for 8 seconds were introduced in the task and were signed by a black square (“▪”). The number of target (letter included in the memory set) and non-target (letter not included in the memory set) probes was balanced across the task. The task design is shown in Fig. 5.
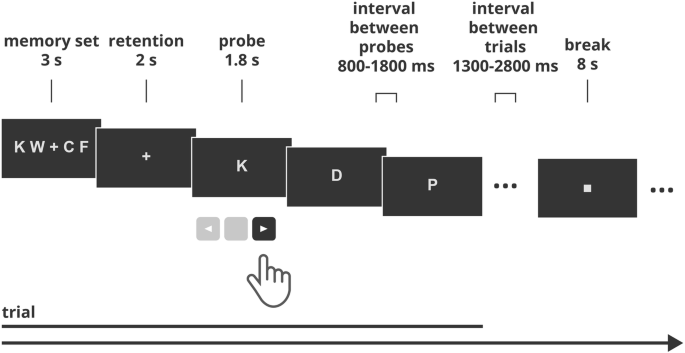
Sternberg’s task design. A sample trial of the non-demanding condition is shown. The “K” letter is the target.
Information regarding the basic analysis
All statistical analyses were performed using Jeffrey’s Amazing Statistics Program (JASP) (v.0.17.0) (JASP Team, 2023). For quantitative variables (reaction times), a paired t-test was used if the condition of normality of distribution among groups was met (Leven’s test). In case of violation of this condition, a non-parametric Wilcoxon signed-ranks test was used. The boxplots were prepared with Seaborn Python Library.
Resting-state session
A resting-state protocol was used to study spontaneous brain activity when no specific task was given. It allows for the study of, among other questions, brain functional connectivity. During the EEG session, subjects were instructed to remain still and quiet, firstly with the eyes open (for 4 minutes) and then with the eyes closed (for 6 minutes). Both conditions were saved in one file. During the fMRI session, a closed-eye condition was used that lasted for 12 minutes.